

Currently available presbyopia-correcting IOLs increase patients’ depth of field but typically reduce the quality of vision and increase night vision symptoms or photopsias. The goal of this article is to explain how these interrelated qualities affect patients.
UNDERSTANDING PHOTOPSIAS
Night vision symptoms can be divided into three types: glare/flare, halos, and starbursts. Although these terms are often used interchangeably, and the photopsias can occur in combination, each represents a distinct effect with a particular cause. Glare/flare is a blurring or smearing of lights, halos are distinct rings around lights, and starbursts appear as rays or streaks coming from lights (Figure 1). In pseudophakic patients, glare and starbursts generally result from posterior capsular opacification (PCO), refractive error (eg, astigmatism), optical aberrations, and/or problems with the tear film or ocular surface. Halos are typically related to multifocal IOLs.
Mechanistically, photopsias result from off-axis light. The pattern and amount of off-axis light energy correlates to the shape and intensity of the photopsia.
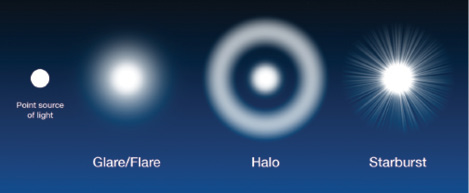
Figure 1. There are three distinct types of photopsias or distortions of a point source of light.
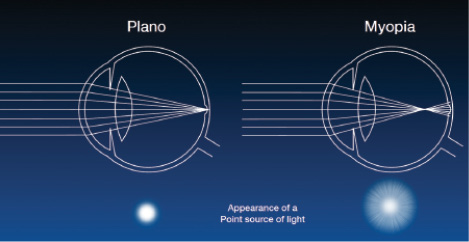
Figure 2. Myopia (and therefore monovision) results in off-axis light and produces glare and starbursts.
In a plano, perfectly focused eye, all the rays from a point source are on axis (Figure 2, left). In the defocused case of myopia, with the focal point in front of the retina, light rays diffuse when they hit the retina. Because light rays end up off axis in a myopic eye, glare and starbursts result (Figure 2, right).
ADD POWER, OPTIC DESIGN, AND HALOS
The defocus curves for presbyopia-correcting IOLs plot visual acuity over a range of near defocus. Because visual acuity is related to light energy, it is possible to predict the size, shape, and brightness of photopsias from the shape of the defocus curve.
For example, a multifocal IOL (bifocal in nature) has peaks at far and near and a dip at intermediate. The relatively decreased light energy in the “dip” is what creates the separation between the point source of light and the halo. The amount of add power determines the size of the halo, whereas the height of the peak correlates with the brightness of the halo (Figure 3). A closer near point with greater light energy would therefore result in a bigger and brighter halo.
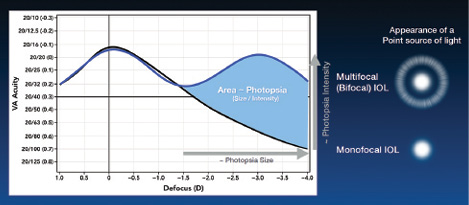
Figure 3. In a presbyopia-correcting IOL, the amount of add power (horizontal arrow) correlates to the size of the halo, whereas the height of the peak (vertical arrow) correlates to the brightness of the halo.
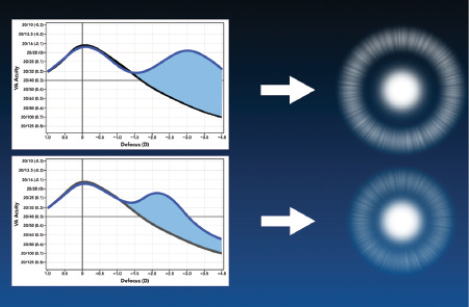
Figure 4. Reducing the add power and directing less energy to near can make the halo a little smaller and dimmer but result in less near vision.
If the add power is reduced or less energy is directed to near vision, as in the bottom of Figure 4, the halo would be smaller and dimmer. For example, the apodized diffractive Acrysof IQ Restor IOL +3.0 D (Alcon) directs less energy to a less proximal near focus than the fully diffractive Tecnis Multifocal +4.00 IOL (Abbott), so with the resulting reduction in near acuity, a smaller and dimmer halo would be expected with the Restor.
If the energy distribution between far and near is kept constant, reducing the add power in low-add multifocal IOLs has a direct and predictable effect on night vision symptoms—smaller halos. For example, the rays for the near focal point from a +2.75 D add Tecnis Multifocal IOL (ZKB00) is less out of focus than for the +4.00 D add Tecnis Multifocal IOL (ZMB00), so the halo is correspondingly smaller. Smaller halos are less likely to block the view of surrounding objects and are therefore better tolerated by patients.
ACHIEVING A BETTER BALANCE
Having more options allows surgeons to personalize presbyopic treatment for each patient. Lowering the add power predictably increases patients’ satisfaction with their vision at night.
In the clinical trials for the low-add Tecnis Multifocal IOLs, it was noted that 89% of +2.75 D add (ZKB00) patients and 87% of +3.25 D add (ZLB00) patients were completely or mostly satisfied at night compared with only 84% of those with the monofocal (ZCB00) IOL. It appears that, when symptoms are reduced, patients can tolerate minor photopsias for the gains in near vision they want.
However, balancing presbyopic correction and night vision symptoms is not as easy as simply minimizing photopsias. In the monovision state, more light is off axis than with any presbyopia-correcting IOL, yet many patients do well with monovision. Perhaps the discreet nature of halos contributes to their symptomatic intolerance.
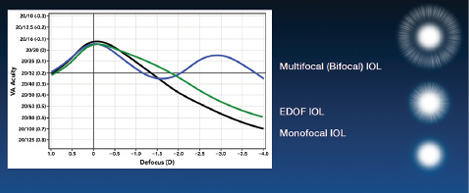
Figure 5. Simulated halo effects for a theoretical monofocal IOL, multifocal IOL, and EDOF IOL.
A new category of IOLs, known as extended-depth-of-focus (EDOF) IOLs, have a monotonically declining defocus curve. Instead of an inflection point with a second peak (as with multifocal IOLs), the EDOF curve is more like that of a monofocal lens but with a broader peak and therefore good vision over a wide range of defocus. In theory, these IOLs have less off-axis light and thus are associated with fewer night vision symptoms than multifocal IOLs (Figure 5).
CONCLUSION
These concepts that relate near vision with photopsias can help surgeons to explain night vision symptoms to patients interested in presbyopic correction. Additionally, surgeons now have a better grasp of what new technology will bring. With the recent FDA approval of the Tecnis Symfony IOL (Abbott), ophthalmologists now have a first-in-class EDOF IOL. The unique defocus curve of the Tecnis Symfony provides surgeons with a new and possibly better way to balance visual quality, depth of field, and night vision symptoms. With a proper understanding of how these quantities are related, surgeons are now more equipped than ever to provide the quality and range of vision that patients desire.
Daniel H. Chang, MD
• private practice at Empire Eye and Laser Center in Bakersfield, California
• empireeyeandlaser.com
• (661) 325-3937; dchang@empireeyeandlaser.com
• financial disclosure: consultant to Abbott

