

Presbyopia-correcting IOLs have been a part of ophthalmologists’ armamentarium since the FDA’s 1997 approval of the Array multifocal lens (Abbott Medical Optics [AMO]). The category of IOLs really took off, however, in the mid-2000s with the availability of accommodating IOLs as well as newer generations of multifocal IOLs. During the past decade, the emphasis in presbyopia-correcting IOLs has shifted toward higher-quality distance vision. Many surgeons have told this author that their use of the Crystalens/Trulign platform (Bausch + Lomb) has grown significantly. These accommodating lenses emphasize distance and intermediate acuity at the expense of high-grade near vision.
The manufacturers of multifocal IOLs are intent on increasing their market share. This year brought the introduction of three new multifocal lenses in the United States, all of which emphasize better-quality distance vision than earlier generations of this technology and address the increasing demand for good intermediate vision brought on by the growing popularity of handheld electronic devices.
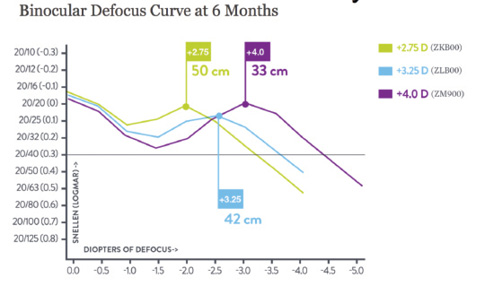
Figure 1. The Tecnis Multifocal IOL is available in three different add powers, allowing selection of the near zone.
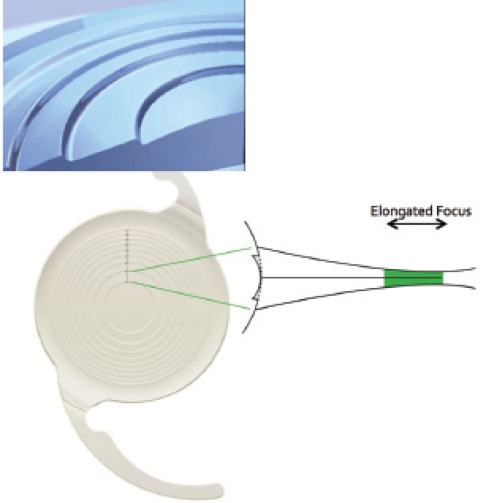
Figure 2. The Symfony IOL uses diffractive ridges to create a single elongated zone of focus as opposed to the two zones of focus typically found in a multifocal lens.
THE LATEST MULTIFOCAL LENSES
In 2015, Alcon released a new version of its popular multifocal IOL that has a 2.50 D diffractive add. The AcrySof IQ Restor IOL +2.5 D features a larger central refractive zone as well as fewer diffractive rings than other models of this lens. As a result, more of the available light energy is directed toward distance vision at all pupillary diameters. Clinically, this translates into better distance and intermediate vision while sacrificing some very close near vision. For many patients, it is a welcome trade.
New models of the Tecnis Multifocal IOL (AMO) also address the need for better intermediate vision, effectively allowing surgeons to select the range at which a patient will see for near. In addition to the previously available 4.00 D model, 3.25 and 2.75 D versions are now available with corresponding zones of best near vision at 33, 42, and 50 cm (Figure 1). In the FDA trial, 96% of patients receiving the 3.25 D lens bilaterally were able to function without glasses at distance and intermediate ranges, and 94% said they would elect to receive the same IOL again. For the 2.75 D model, 98% of patients were able to function without glasses at distance and intermediate, and 97% said they would elect to receive the same IOL again. Six months postoperatively, 84% of patients with the 3.25 D lens and 91% of those with the 2.75 D model reported no problems driving at night.1
ON THE HORIZON
Designs in development offer the tantalizing prospect of crisp uncorrected near and intermediate vision combined with optical performance at distance rivaling that provided by a monofocal IOL. Can this be achieved? If so, it would disrupt the way ophthalmologists approach IOL surgery.
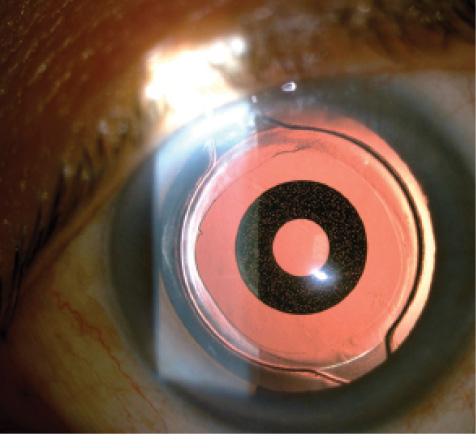
Figure 3. The IC-8.
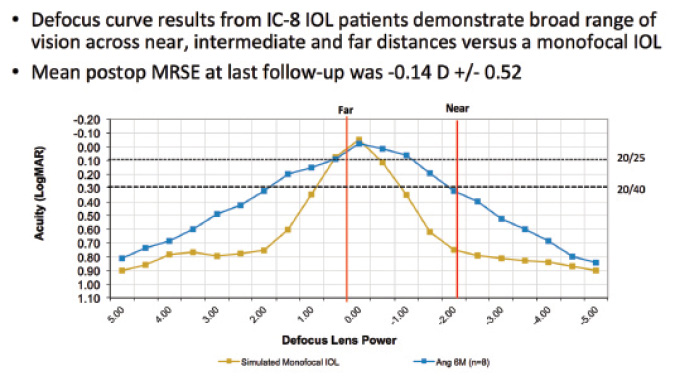
Figure 4. The IC-8 provides near vision by dramatically extending the depth of focus compared with a standard monofocal IOL (R. Ang, MD, unpublished data, 2015). Abbreviation: MRSE, manifest refraction spherical equivalent.
Symfony IOL
A so-called extended-depth-of-focus IOL, the Symfony IOL (AMO) uses three principal optical strategies to achieve good near vision. First, it incorporates negative spherical aberration to counteract the positive spherical aberration typically found in the cornea. Second, it features diffractive ridges that physically resemble those found in a multifocal IOL, but the Symfony is not a multifocal. Instead, the diffractive ridge pattern extends the size of a single zone of focus (Figure 2). Third, the Symfony takes advantage of the way lenses induce chromatic aberration. Owing to the prismatic effect of all refractive lenses, various wavelengths of light are bent differently: blue, short wavelengths are bent more than long, red wavelengths. With a diffractive optic, the situation is exactly the opposite: blue, short wavelengths are bent less than long, red wavelengths. In the Symfony, these two factors cancel each other out, resulting in control of chromatic aberration (data on file with AMO).
In a study of 31 patients bilaterally implanted with the Symfony IOL, the mean distance and intermediate UCVA was 20/20, and patients demonstrated this same level of acuity through 1.50 D of defocus (data on file with AMO). In other words, one could refract these patients to 20/20 and then place an additional 1.50 D of negative sphere in front of their eye, but the acuity would remain 20/20. Importantly, there were no significant differences in night vision complaints between Symfony patients and monofocal IOL controls.
IC-8
Another intriguing IOL in development comes from AcuFocus, maker of the Kamra corneal inlay. The IC-8 features a mask similar to a Kamra inlay placed inside the optic of a monofocal IOL (Figure 3). The IC-8’s mask has a slightly smaller aperture of 1.36 mm versus 1.6 mm for the Kamra. The purpose of the mask is to dramatically expand the depth of focus through the pinhole effect, resulting in good near UCVA. Initial data (R. Ang, MD, unpublished data, 2015) from outside the United States look promising (Figure 4).
CONCLUSION
Currently available presbyopia-correcting IOLs provide remarkable clinical outcomes, and the vast majority of patients achieve highly satisfactory results. The demand for improved visual quality will drive the development of better and better designs, which will increase surgeons’ ability to tailor the technologies they use to the specific visual goals of each patient. n
1. Updated DFU for the Tecnis Multifocal Foldable Acrylic Intraocular Lens. Abbott Medical Optics. 2014. http://www.accessdata.fda.gov/cdrh_docs/pdf/P980040S049d.pdf. Accessed August 19, 2015.
Steven J. Dell, MD
• medical director, Dell Laser Consultants, Austin, Texas
• chief medical editor, CRST
• (512) 327-7000
• financial disclosure: consultant to AMO and Bausch + Lomb

